Radionics ~ Part II
 by The Radionist (Journal Of Borderland Research)
by The Radionist (Journal Of Borderland Research)
As Dr. Abrams’ practice grew, spurred by the increasing accuracy and thoroughness of his diagnoses, more and more instances arose of patients who wished to avail themselves of his method but who could not visit his office, either because they were too ill to make an office visit, or lived too far away. In the effort to be of service to these individuals, experiments were made with blood specimens taken from people who were ill, and placed in a metal cup (which Dr. Abrams termed a “dynamizer”), with connecting wires to the head and foot plates attached to the healthy subject (reagent) on whom the percussion diagnosis was performed. It was found that the blood carried all the radiations of the body from which it had been drawn, and could therefore be used as a substitute for the presence of the patient in the examining room. With the blood in the metal cup connected to the healthy subject, the diagnostic tests performed on that subject produced the same tunings and measurements as those prevailing when the patient (from whom the blood had been drawn) was personally connected to the reagent, through the tuning controls.
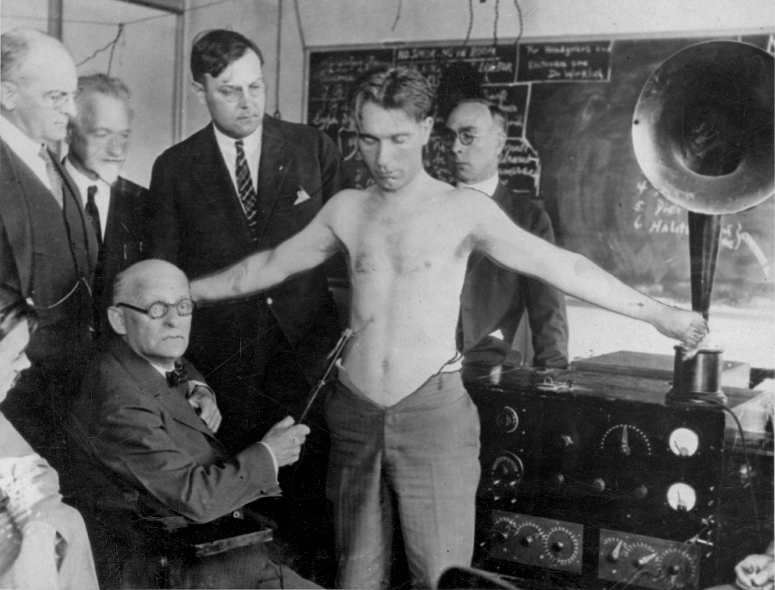 Dr. Albert Abrams demonstrating his E.R.A. system (~1923)
Dr. Albert Abrams demonstrating his E.R.A. system (~1923)
Since the blood flowed through every organ, gland and tissue of the body, it was reasonable to assume that all the radiations from those organs, glands and tissues would be absorbed by the blood including the radiations of any diseases present. This theory was later proven independently by the blood crystallizations method developed by the late Dr. Ehrenfried Pfieffer. He perfected a technique for evaporating a small amount of blood in a copper sulphate solution. Crystalline patterns were formed, each different disease resulting in a different pattern.
The blood came to be used in the E.R.A. (Electronic Reactions of Abrams) method (and later in radionics by some of the practitioners), in dried form, on a piece of blotting paper or other absorbent paper; this is in contrast to laboratory procedures, for which the blood is used, in liquid form. Since liquid blood spoils rapidly, it has to be mixed with a quantity of preservative. For the purpose of E.R.A. or radionic tests, a preservative must not be used, since it adds a strong foreign vibration or radiation of its own. Since dried blood serves equally well as liquid blood for the purpose of E.R.A. or radionic tests, the blood came to be used in dried form to avoid the use of preservatives.
The use of blood specimens broadened the utility of E.R.A. method but introduced special problems. One of the problems was that of contamination. Both the E.R.A. and the radionic method are extremely sensitive, to the extent that if someone other than the patient handled the piece of paper on which the patient’s blood specimen was placed, even a very slight amount of skin perspiration from the other person would place that person’s radiations into the paper, to a degree. The result was that the practitioner would then likely detect the combined radiations of the two individuals — the patient, and the Doctor or other person who had handled the specimens. This of course led to detecting and reporting of ailments or conditions not present in the patient. When this was discovered, special precautions were laid down for the preparation of blood specimens, to keep them free from contamination. However, those who would try to trick the practitioner were not interested in observing such precautions.
Another disadvantage of the use of blood specimens lay in the fact that the door was opened to trickery of various kinds. For example, blood specimens from animals and poultry were sent to the Doctor, ostensibly as human blood specimens. When the reports came back listing the various diseases found, the method was derided and ridiculed. Actually, the same trick can be successfully perpetrated on medical laboratories, since the laboratory work required to perform blood counts does not disclose whether the specimen is from a human or from an animal! The blood count ranges differ somewhat, but only to the extent that a reading that would be normal for some of the animals occurs frequently in humans who are ill. Animals and poultry are subject to the same toxic and infectious diseases as are humans; primates have the same organs and glands as do humans, quadrupeds have most of the organs, glands and other structures of humans. Poultry are now being used as the subject of spin tests in the astronaut program “because their circulatory system is so similar to that of humans”. The reports of disease radiations found in the animal specimens did not in the least invalidate the method, but those unskilled in a new field are quite prone to unthinkingly accept adverse criticism that seems logical on the surface.
In modern radionics there are tuning rates to differentiate human and animal specimens; however this requires extra checking and so are not always used.
EVOLUTION OF THE DETECTION METHOD
In the evolvement of the Abrams method of detecting disease radiations, the next step taken was the abandonment of the percussion tests, and in their place the adoption of the method of rubbing or stroking the abdomen of the healthy subject, with a glass rod. The percussion method of eliciting the signals or responses required a very high degree of skill, and was too difficult to teach to others. The use of the glass rod, while not easy to learn, at least proved possible for some others besides Dr. Abrams. In the use of the rod, the ease with which it slipped over the abdominal surface was noted. A significant manifestation occurred when the rod appeared to “stick” over a particular abdominal area, where more energy or force was required to move it a given distance on the skin of the subject. This phenomenon of “sticking” occurred in conjunction with tunings for disease and would disappear when the volume measurement control was advanced to a setting indicative of a strength of radiation greater than that which was being received.
COLORED LIGHT AND DISEASE
A further development was the addition of colored lights to shine on some element of the detecting circuit. These were said to have been originally suggested to Dr. Abrams by a Dr. McManus, an osteopath from Kirksville, Mo. The original colors used were red, yellow, green and blue, in addition to incandescent light of nonspecific color, termed “white light”. A selector switch was incorporated, permitting the use of any one of those lights, or the use of no light. The reason for the use of colored light was because it was found that certain disease radiations manifested more strongly in the presence of specific colors of light. Thus the TB radiation was stronger and more easily detected when the red light was used; staph. radiation was stronger when the blue light was on; strep. was more readily detected with green light; and inflammation came in more clearly when the yellow light was used. Bacteria, cold or flu toxins manifested better when white light was turned on.
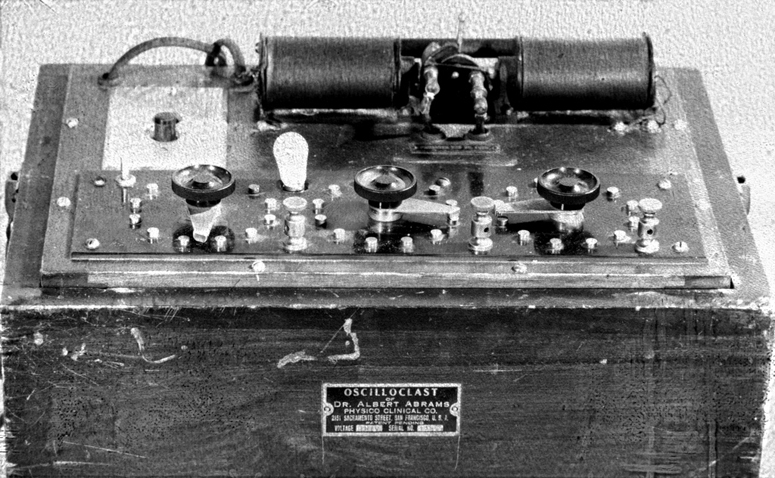 “Oscilloclast of Dr. Albert Abrams” — FDA
“Oscilloclast of Dr. Albert Abrams” — FDA
We have seen that the evolvement of the detection method of E.R.A. arose mainly through Dr. Abrams’ endeavors to improve his techniques of physical diagnosis, with the direction of these endeavors influenced by Professor de Sauer’s concepts. In contrast, the development of the Abrams treating equipment was from the start a project directed specifically toward the goal of neutralizing or eliminating disease radiations by electronic means.
Dr. Abrams was convinced that the most effective treating current would have to be low enough in amplitude to avoid heating the body tissues and also would avoid causing any pain or discomfort. A further feature of the equipment was that it should be capable of being tuned to the radiational frequency of the specific disease to be overcome. This was a major advance in therapy. The Abrams treating equipment operated in the short-wave band, but differed from short-wave diathermy in many ways, including the following:
- Short-wave diathermy uses heavy power which heats the body tissues. The Abrams treatment equipment purposely avoided heating up the tissues.
- Short-wave diathermy operates on one frequency only. The benefits or advantages of tuning or frequency selections are lost when enough power is applied to heat the body tissues. The Abrams equipment incorporated the beginning of the principle of tuning the treatment current to influence the disease radiation, by offering a choice of eleven different frequencies.
- Short-wave diathermy current is not interrupted. Interruption of such heavy treating current, which has for its goal the production of heat, would slow down the heating of the body, and require longer treatments. In contrast, the Abrams equipment used an interrupted or pulsed current, for better results in therapy.
- Another difference lay in the high degree of damping of the current from the Abrams equipment.
Several parts of the short-wave band were used by Abrams and his immediate successors at different times, but most of the work was done in the lower third of the 43-megacycle band. In the Oscilloclast, the final form of the Abrams treating instrument, the eleven treatment frequencies (from which the operator selected one at a time by means of push-buttons) were in the range of 43.000 megacycles to 43.357 megacycles. (This is in the 10-meter band of very high radio frequencies and just below the television bands. Channel 2 starts at 54.000 megacycles.) Some of these eleven frequencies were designated for the treatment of specific diseases or groups of diseases, as the result of correlations found between disease emanations and short-wave radio frequencies in the detection research. The other treatment frequencies were for the stimulation of function of major organs such as the liver and spleen. It was considered that an interrupted current was more effective than a continuous current, with the combination of high frequency and low power used.
For over twenty years the Abrams treating equipment used mechanical means of interruption of the current output, termed the “tic toc” apparatus, due to its similarity to the pendulum of a clock. The mechanical making and breaking of the circuit produces periodic sparks. The spark itself is known to have some therapeutic value, as witness the Lakhovsky multi-wave oscillators, and the S. S. Knight machines.
In 1958, quite a few years after Dr. Abrams’ death, when radio circuitry with vacuum tubes had become well established, the mechanical means of interrupting the treatment current was abandoned by the Foundation carrying on Dr. Abrams’ work. From then on, the current instead was chopped or pulsed electronically, by an oscillating circuit using vacuum tubes and a condenser. The condenser discharged periodically. There were some practitioners who felt the earlier Abrams treating units using the mechanical make and break were superior.
When the Abrams treatment equipment was in use, the output current, at low voltage and very low amperage, was conducted to the patient by connecting wires attached to metal electrodes placed dry on the patient’s skin. Besides the pulsed, damped short-wave treatment output, variable in tuning to the extent already mentioned, the apparatus also delivered another type of treating current — namely an alternating magnetic current, applied through a separate set of electrodes.
The Abrams treatment instruments, the Oscilloclast and the Oscillotron, are now of interest more for their historical than for their therapeutic value. While they undoubtedly produced some favorable results in many cases that had not yielded to orthodox methods, the length of time and number of treatments required to produce a given result were far greater than for modern radionic equipment. The differences between Abrams treatment equipment and radionic treating units will be outlined in a later installment of this series.
DEVELOPMENT OF THE RUBBING PLATE OR DIAPHRAGM
From the time Dr. Abrams gave his first class to doctors in the use of the E.R.A. diagnostic method in the middle of the second decade of this century, efforts started on the part of some of his followers to see if the use of the human “reagent” could be eliminated. There were three disadvantages to the use of the reagent (healthy subject on whose abdomen the responses were elicited); these disadvantages were of three types — technical, human and financial. The technical problem lay in the difficulty of finding a person who was completely healthy, free of toxicity, with all organs, glands and types of tissue functioning at par. Any deficiency of function, disease radiation or toxicity in the reagent, would be combined with the reactions of the patient, so that the responses would be a mixture of the factors from the two individuals, instead of solely from the patient.
The human problem lay in the fact that very few individuals were willing to stand for long periods of time with abdomen bared, while submitting to the percussion procedure or the stroking of the abdominal skin repeatedly with glass or plastic rods for the purpose of compiling the patient’s electronic analysis data. The economic or financial factor was the necessity for paying for two individuals’ time for each analysis — that of the doctor or other person who operated the equipment, and that of the reagent on whose abdomen the reflex indications were detected.
Dr. Earl Smith, one of those who took Dr. Abrams’ first class in E.R.A. method, reasoned “What is the difference between rubbing a glass-rod on the skin, or rubbing the skin over a piece of glass?” From this question, experimentation began on a set-up in which the operator used his own skin for the purpose of detecting the radiations involved, specifically, the skin of the underside of the operator’s fingers, particularly the balls of the finger-tips and the areas just back of the balls. These skin areas were used for the purpose of stroking the glass plates or slides. The patient’s radiations were conducted to the glass by means of a connecting wire or wires from the tuner, leading to a metal coin or disc placed underneath the glass plate. It was found that glass had to be covered with a certain type of coating, in order that the “stick” could be obtained in accordance with appropriate settings of the tuning and volume-measurement controls in relation to the patient’s radiations.
Various substances for the coating were tried, including india ink, photographer’s re-touching fluid, photographic emulsions, etc. Later it was found that other substances could be used instead of a glass plate; these tried included rubber, leather, wood, and plastic. Rubber was difficult to learn to use, though once mastered, some operators liked it. Leather gave a strong “stick” but required a heavy stroke. Some plastics were very sensitive and gave a stick easily, but also had the fault of giving false sticks — that is, signals when none should have been given. Certain fine-grained hardwoods were preferable, at least for many of the operators. For this purpose, mahogany and manzanita were fairly good. Brazilian rosewood or macumba were among the best. (Rosewood fingerboards are common on stringed musical instruments.)
While the stroking of the reagent’s abdomen with a rod was not quite as difficult as the original Abrams method of diagnosis by percussion, it still was quite far up in the scale of difficulty, and very few could be found who could be successfully trained in the method. A good rubbing plate assembly was noticeably less difficult to learn to use, hence it became possible to enlarge the field of practice to include more substantial numbers of practitioners. The rubbing plate became an integral feature of radionic equipment, while E.R.A. retained the use of the reagent. The E.R.A. method has died out since the Electronic Medical Foundation went out of existence some years ago (the organization to which Dr. Abrams willed his fortune, for carrying on his work). Radionics continues to be used openly and freely in England, to a lesser extent in some other European countries, and on a reduced scale in the United States due to pressures brought to bear against it in recent years by the forces of orthodoxy.
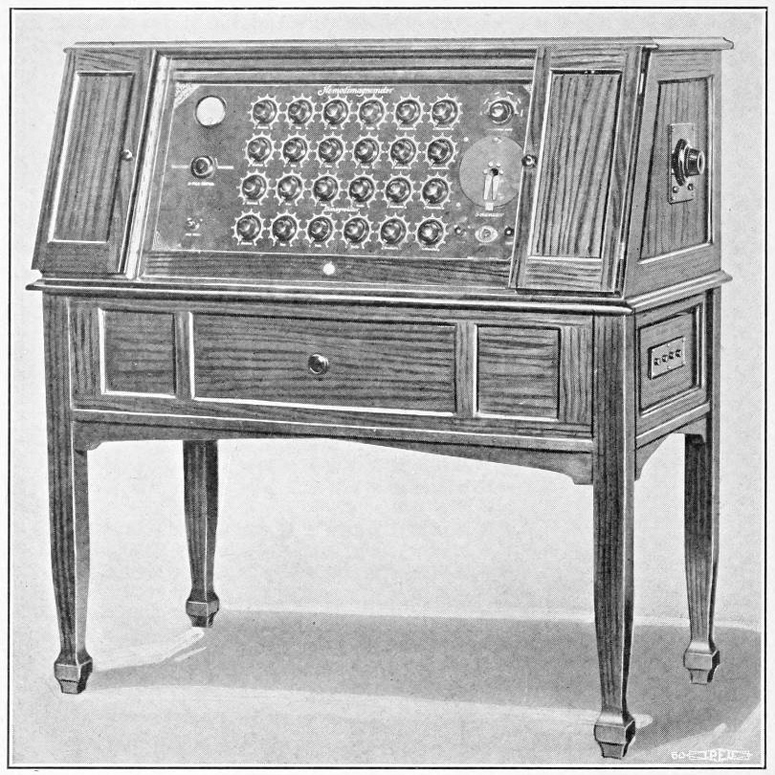 Calbro Magnowave, Inc. “Hemodimagnometer / Dimagnometer”
Calbro Magnowave, Inc. “Hemodimagnometer / Dimagnometer”
The second half of the decade of 1920-1930 witnessed the development of four types of radionic equipment, all more advanced than the Abrams E.R.A. apparatus, and each having its own particular features. These four types were:
- The Calbro Magnowave
- The Pathoclast
- The Radioclast
- The Drown equipment
Each of these types will be described in this series, as they all played a part in the development of the art.
The Calbro Magnowave had the greatest tuning scope of any of the four, including on its tuner panel. Four horizontal rows of tuning dials, six dials per row, giving a total of 24 dials. This permitted the use of more advanced technique than could be utilized on the other types of equipment. Other features of the Calbro Magnowave:
- A rubbing plate warmed by a built-in, low power electric heating element. It was found easier to elicit signals on a rubbing plate kept warm.
- A slotted-screw adjustment for tuning the rubbing plate assembly.
- A button which, when pressed, would clear the instrument of all accumulated radiations. This sometimes was of help to avoid carry over of radiations from one condition to another, and was always of use when changing from one patient to another.
- A specimen well into which a test vial containing a sample of a vitamin, mineral, food or remedy could be inserted, to ascertain what effect the radiations from the test substance would have upon the patient’s organ functions and disease readings.
- A treatment circuit which for the first time used the same type of tuning for treatment as for the diagnostic procedures. This permitted the art of radionic treating to be developed to a far higher peak of selectivity and effectiveness. It opened the door to a tremendous variety of treatment effects, such as had never been known previously. Most of the remainder of this installment will be devoted to the treatment aspect of the Calbro Magnowave.
Previous use of radionic treating had been on the basis of one tuning for each type of disease. However it was learned that, for example, strep in the liver required a different treating rate for effective elimination than for strep in the thyroid, and similarly a different treating rate was required for treating that bacteria out of each different organ or gland in the body. Also, the treatment rate that will most effectively eliminate strep (to continue to use an example) from one person’s liver will not be the rate that will most thoroughly eliminate it from another person’s liver! Every individual has different bio-chemical and electro-chemical reactions, just as every individual has different finger-prints and foot-prints. These differences mean that only by individualized or personalized adjustment of treatment tunings can the quickest and most thorough results be obtained.
The prime virtue of the Calbro Magnowave is that for the first time it permitted the utilization of “personal” treatment rates, individually developed for each patient, for the most thorough elimination of disease factors from specific organs, glands or other tissues of that particular person. This was done by providing pre-precise matching of individual bio-electric radiations in specific organs of the person, as altered by specific disease factors. This introduced a degree of precision into therapeutics which far outmatched anything available in medical practice to this day.
Personal treatment rates are only possible when the tuning apparatus in the treatment circuit is of the same type as used in the diagnostic circuits. Also, personal treatment rates cannot be satisfactorily used on instruments of limited tuning scope such as the Pathoclast or Drown instruments, and most of the Radioclast models. With the Calbro Magnowave, and successor instruments to be described later, the operator first performs the diagnostic analysis and determines which organs require treatment and also determines what disease conditions should be eliminated. Usually there is more than one disease condition or type of tissue pathology, and more than one organ that needs attention. Choosing the condition and organ to be treated first, the tunings for the condition and the organ are placed on the tuner panel, the intensity of the adverse condition in that organ is noted, then the tuning dials on the treatment row are brought into play, from one end of the row to the other, the operator determining for each dial the setting that will best neutralize the disease condition in the organ or location involved. This determination is made by means of resonance detected on the rubbing plate, which is used constantly during the period of time in which the operator is developing the personal treating rate.
The procedure is not automatic, and results vary with the skill of the operator. Assuming a competent, skillful operator, the procedure opened up a whole new field of therapy. It permitted conditions to be cured which hitherto could not be touched — examples will be given toward the end of this series. Right now, the nature of the treatment current should be mentioned.
In contrast to the Abrams Oscilloclast, which used a small number of short-wave radio frequencies for treatment, the Calbro Magnowave and successor instruments used the emanation from one side of the 110-volt house current, tuned radionically by the treatment row of tuning dials.
In conventional electricity it is not generally known that a current can be obtained from one side of the electric line — from the “hot” side only. However, the fact that such a current is obtainable is known to some radar experts, as it is a disturbing factor in radar. The presence of such a current can be readily demonstrated with a 1/25th watt neon test bulb: connecting one terminal of the bulb to the hot side of the alternating current line, the bulb will light dimly when its other terminal is touched with the finger.
This current, obtainable from one side of the alternating current line, is extremely low in magnitude; thus it does not disturb or upset the normal flow of nerve energy in the human being. It is therefore an ideal carrier wave for the subtle effects of the tunings introduced by the radionic treatment dial settings — effects which would largely be lost or seriously overwhelmed by more gross electrical currents such as the sine wave or faradic.
Any Calbro Magnowave instruments that may still be in existence inevitably have badly corroded, worn or loose contacts due to the age of the equipment, and would need to be completely rebuilt in order to function properly.
The first word of the name, “Calbro Magnowave”, was obtained from the last names, Caldwell and Bronson, of the two men who formed the company that developed and made the equipment. The second word was coined. Over a thousand of these instruments were said to have been sold during the late nineteen twenties and early thirties. It was the first radionic instrument to attain such a side sale, and possibly the only one that did so. A convention of users of the equipment adopted the term “radionic” as descriptive of the equipment, and at the same convention an association of users was formed, termed the “International Radionic Association”, which continued in existence for nearly thirty years.
MAGNETIC FIELD CANCER CURE
“Mice live up to 45% longer after they’ve been subjected to certain types of magnetic fields, and cancerous mice lose their malignant growths after similar treatment, a Los Angeles space scientist said here yesterday. (Los Angeles ‘Times’, April 1960). Dr. Harold S. Alexander of North American Aviation Corp.’s missile division told scientists at an annual meeting of the Institute of Environmental Sciences at the Biltmore that much more research must be conducted before the effect of these magnetic fields on humans will be known.
“But, he said, several leading cancer researchers are already pursuing the experiments pioneered by Dr. Jeno Barnothy, Hungarian physicist now of Chicago, who participated in yesterday’s program.
“‘Aside from the effect on malignancies (cancer), we don’t yet know why the mice live so much longer after four to six weeks in a magnetic field,’ Dr. Alexander said, ‘but we think the experiments have some effect on the rate of cellular reproduction.’
“He displayed photographs of two mice from the same litter which had reached an age equivalent to 90 years in humans. The one which had lived for awhile in a magnetic field appeared only about one third as old as the other.”
The California Medical Association has now had over eight years to research this spectacular cancer-cure breakthrough, but so far only thunderous silence.
See Part I here. See Part III here.

Related posts:



Posted in Health, Other Topics, Science For The New Agewith comments disabled.