Radionics ~ Treatment And Diagnosis Using Radiations Of Energy
 by The Radionist (Journal of Borderland Research)
by The Radionist (Journal of Borderland Research)
To start with a definition — Radionics is an art by which diagnostic data is obtained through use of equipment which enables a trained operator to detect and measure differential radiations by the different organs and tissues of the body. Other uses of the equipment include detecting, ascertaining the location in the body, and measuring the amplitude of various types of pathology and adverse conditions of tissue, and similarly to detect, locate and measure any foreign micro-organisms, parasites, and other irritant factors that contribute to disease. Also the use of the equipment for resonance tests by which the effect of any proposed remedy such as a vitamin, mineral, homeopathic substance or nutritional concentrate can be predetermined with regard to any organ, system or function of the body. Last but not least, the administration of subtle forms of energy for treatment.
These treatment energies are of sufficiently low power to approximately match the level of amplitude of the body’s own nerve currents; their unique feature, which differentiates them from all other forms of electrical or electronic therapy, is that they can be modified through a very wide range of tuning so as to selectively affect any organ, gland, or type of tissue desired — either to stimulate under-active function or inhibit over-active function. The treatment energies can also be tuned to neutralize or cause the body to excrete harmful deposits or accumulations of irritant substances or microorganisms, with specific tunings for each different substance or type of micro-organism. The effects of or results from the use of radionics varies from outstanding and even phenomenal success, through a scale of fair or mediocre results, down to a lack of benefit, depending entirely on the equipment used, the techniques applied, and the level of skill and understanding of the operator. It is the purpose of this series to give an outline of the history of radionics, the different types of equipment that have been developed and used in this field, their advantages and weak points, and to discuss in condensed form both the benefits that have been obtained from radionics and the problems involved in its use.
To understand the origin of radionics, one must first look into its predecessor, E.R.A. These letters stand for the Electronic Reactions of Abrams, Radionics is not the same as E.R.A., but is an outgrowth of it. Without E.R.A. there would probably have been no radionics.
 “Dr. Abrams and His Electrical Disease Detector”
“Dr. Abrams and His Electrical Disease Detector”
THE RADIATIONAL NATURE OF DISEASE
The originator of E.R.A. was Dr. Albert Abrams, M.D. of San Francisco, California. He was born Dec. 8, 1865 and died Jan. 13, 1924. He obtained his medical education at University of Heidelberg in Germany — the country which at that time led the world in medical advancement. He took postgraduate courses in London, Berlin, Paris and Vienna. In fact he was one of the most highly trained medical physicians of his time. He held numerous posts of honor; there were many publications to his credit; and he was held in the highest respect and admiration by the medical profession of the United States up until the time that he propounded the theory of E.R.A. That theory was so far in advance of the thinking of his period, that he then became a lonely figure in the medical profession of the United States, though the profession in England was more open-minded in its approach to E.R.A.
Late in the 1800s, when Dr. Abrams was taking post-graduate work at University of Heidelberg, he studied under a Professor De Sauer, who lectured extensively on the concept of the radiational nature of disease. Dr. Abrams was so impressed with those lectures that upon his return to California he embarked on an extensive series of experiments to test the validity of Professor De Sauer’s theories. The results of numerous experiments convinced him that those theories were correct. The following are some of the experiments as illustrative examples:
A test-tube of TB bacillus culture, held by means of adhesive tape to a location over the 3rd and 4th dorsal spinal segments of a healthy person, produced blanching of the face that was typical of a tubercular. Upon removal of the test-tube of culture, blanching ceased.
Dr. Abrams diagnosed tumors by a characteristic dull sound elicited by percussion upon certain areas of the patient’s abdomen. Patients without tumors did not manifest the dull sound.
After diagnosing a tumor in a patient in this manner, the growth was removed by surgery, and then strapped to the forehead of a healthy person. Thereupon, that individual exhibited the same diagnostic dull sound upon abdominal percussion, that had manifested in the patient from whom the tumor had been taken! Upon removal of the tumor from the healthy person’s forehead, the dull sound disappeared.
The phenomena involved in these and numerous other experiments, pointed directly to the radiational nature of disease. The test-tube of TB bacillus radiated something into the healthy subject’s body, that induced a TB symptom. Radiation from the tumor tissue produced a diagnostic signal indicative of a tumor, so long as the tumor tissue was within radiational range of the healthy subject. The evidence from Dr. Abrams long series of experiments was so overwhelming, that he thoroughly accepted De Sauer’s concept, and initiated a program of research and development to produce equipment for practical use of that concept.
ELECTRONIC REACTIONS OF ABRAMS
The first book devoted exclusively to the development of E.R.A. was Dr. Abrams’ “New Concepts in Diagnosis and Treatment”, published about 1916. This followed Spondylotherapy editions referring to E.R.A. — the 5th edition and possibly an earlier edition. Many of the preliminary experiments which led to the development of E.R.A. are detailed in the book “New Concepts in Diagnosis and Treatment”.
In accordance with the results of over a decade of experiments, Dr. Abrams propounded two basic hypotheses:
That all matter radiates, and that the characteristics of the radiations from any type of matter are dependent upon the molecular constituents of the material involved. This means that every different element or compound has a radiation differing from the radiation emitted by any other element or compound.
That the radiations emitted by the different types of matter (and by the different organs of a living organism) can be detected, selectively differentiated, and the radiational amplitudes measured, by a trained operator using relatively simple equipment.
The first hypothesis was in contradiction to scientific principles as understood by the scientific community of Abrams’ time. It was believed then that only the so-called radioactive elements radiated, such as radium, uranium, etc. It was not until after the advent of atomic physics that science evolved to the point where it recognized that all matter radiates. See any scientific text on “magnetic resonance”, including two types: NMR (neutron magnetic resonance), and EMR (electromagnetic resonance). In scientific encyclopedias, one can now look up these subjects and see diagrams and descriptions of elaborate laboratory set-ups that prove the existence of radiation from non-radioactive elements. These laboratory set-ups involve the use of extremes of temperature and pressure (or vacuum), in conjunction with element samples and electrical circuits. There is a different set-up for each element involved. The set-ups are cumbersome and expensive; but at least they prove the underlying principle, first propounded in modern times by Dr. Albert Abrams.
The second hypothesis has not received any general acceptance by the scientific community as yet, although it is self-evident to every successful radionics operator, and to any accomplished radiesthesist.
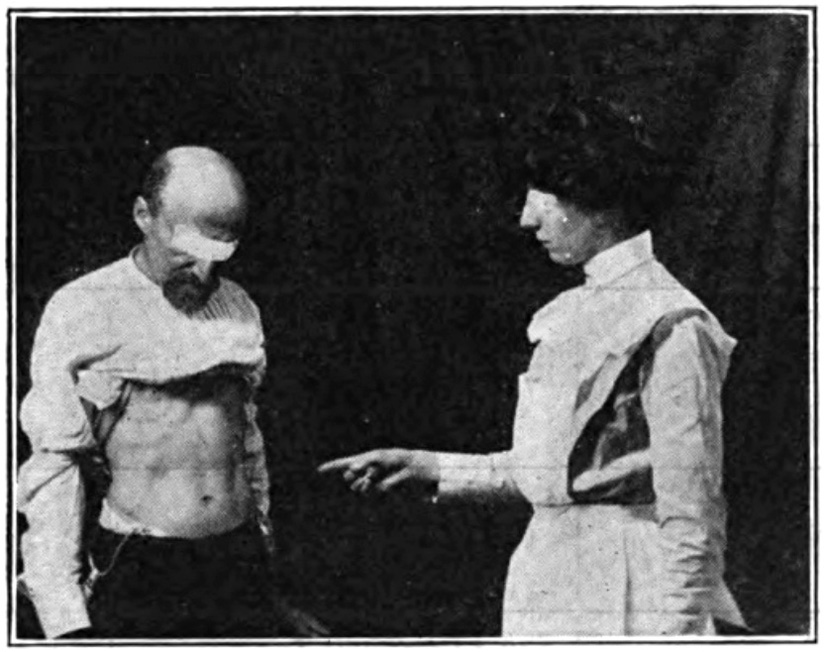 “Illustrating the method of eliciting the stomach reflex” (from Abrams’ “Human Energy”)
“Illustrating the method of eliciting the stomach reflex” (from Abrams’ “Human Energy”)
Dr. Abrams had developed a very detailed procedure for physical diagnosis, with extensive use of percussion and palpation. He particularly emphasized percussion and found correlations between abnormal percussive sounds elicited from specific areas of the abdomen and pathology in particular parts of the body. To put it another way, he ascertained there were reflex connections between specific organs and particular areas of the abdomen. He found there were modifications in the sounds elicited by his percussion tests if syphilis, gonorrhea or TB were present.
The percussion tests had to be made while the patient was standing, facing a particular direction of the compass, with abdomen bared. Dr. Abrams’ physical examination procedure was long and rigorous, and constituted something of an ordeal for patients who were quite ill. In an effort to make the examination easier for patients who were feeling too sick to stand for the required length of time, wires were connected from a metal band on the forehead of the patient to a similar band on the forehead of the healthy person, and from a metal plate in contact with the patient’s feet, to another metal plate on which the healthy person stood with bare feet. With this hook-up Dr. Abrams found he could make his percussion and other tests upon the body of the healthy subject, and the subject then manifested all the disease reactions of the patient. Meanwhile the patient was reclining in comfort on a couch or sitting in a chair.
That the patient’s disease reactions could manifest in the body of a healthy subject, when the two bodies were connected, showed that disease radiations and organ radiations would travel along conducting wires. Thus, no doubt unwittingly, the first step had been taken toward the development of a diagnostic circuit. In his search for methods to sharpen the sounds and thus make his percussion and palpation diagnosis more certain, Dr. Abrams tried the insertion of rheostats in one of the wires leading from the patient to a healthy subject.
The rheostat, a device used to control the amount of current flowing in electrical circuits, consisted of a coil of bare resistance wire wound around a tube or frame bent or formed into a curve. This usually encompassed the greater part of a circle. One end of the resistance wire constituted one of the contacts to the rheostat. The other contact was connected to a slider which by means of a shaft and knob could be rotated. The arm of the slider made contact with the coil of resistance wire in such a way that by turning the knob, the number of turns of resistance wire in the circuit could be increased or decreased, depending on the direction of rotation of the knob and shaft.
DECIMAL READINGS OF INFINITY
The knob had a pointer, which pointed to a curved scale of position settings, on a board or panel. The dial settings of the rheostat showed, essentially, what proportion of the curved coil of resistance wire was included in the circuit. The scale was usually divided into divisions of zero to 100.
With one rheostat inserted into the connecting line between patient and healthy subject, it was found that with a patient who had syphilis, the sounds elicited by percussion on the abdomen of the healthy subject were considerably sharpened when the rheostat in the connecting line between the patient and the subject was set to the position of 55. Similarly, the percussion sounds on the healthy subject’s abdomen were augmented by a setting of 52 if the patient suffered from gonorrhea. Likewise the percussion sounds elicited from the subject’s abdomen were enhanced or augmented by a setting of 42, if the patient connected to the subject through the rheostat was a tubercular. Thus the principle of tuning in to disease was inaugurated. The original experimental work was done with these three diseases since their presence or absence could readily be determined by laboratory tests.
Other tunings were later added for additional diseases, such as flu, strep., staph., pneumonia, etc. Later the tuning range was increased by using two rheostats in series, providing for a total of 10,000 possible positions or settings. Many interesting and valuable discoveries were made by the use of this method; for example, reactions indicative of syphilis, gonorrhea or TB were elicited in patients who had once had one of these ailments, perhaps many years previous, though treatment had suppressed any outward evidence of the disease. The electronic reaction elicited by the Abrams method showed that the disease factor was still present in the body. It was found that in many instances, the patient’s present complaints were eliminated or greatly alleviated when additional treatment was applied to finish clearing the syphilitic, gonorrheal or tubercular factor from the body.
In other cases a smaller or weaker reaction indicative of of one or more of these three basic diseases was elicited in patients who had no medical history of any of those ailments; upon investigation it was learned that a parent or grand-parent or previous ancestor had manifested the ailment for which the electronic reaction was elicited in the descendant. Here again, the health of the patient improved a great deal when treatment eliminated the reaction characteristic of those three basic diseases.
The inheritance of a tissue taint by the descendants of those who suffered from venereal disease or TB is reminiscent of Dr. Samuel Hahnemann’s “chronic miasmas”. Dr. Hahnemann was the founder of Homeopathy. The principle of inherited toxins is thus well known to homeopaths. For them it is a concept accepted on faith, a point of doctrine; but to the electronic or radionic practitioner it is a demonstrated fact. This fact points toward improving health in a way that orthodox medicine cannot provide, since orthodoxy does not recognise the underlying condition.
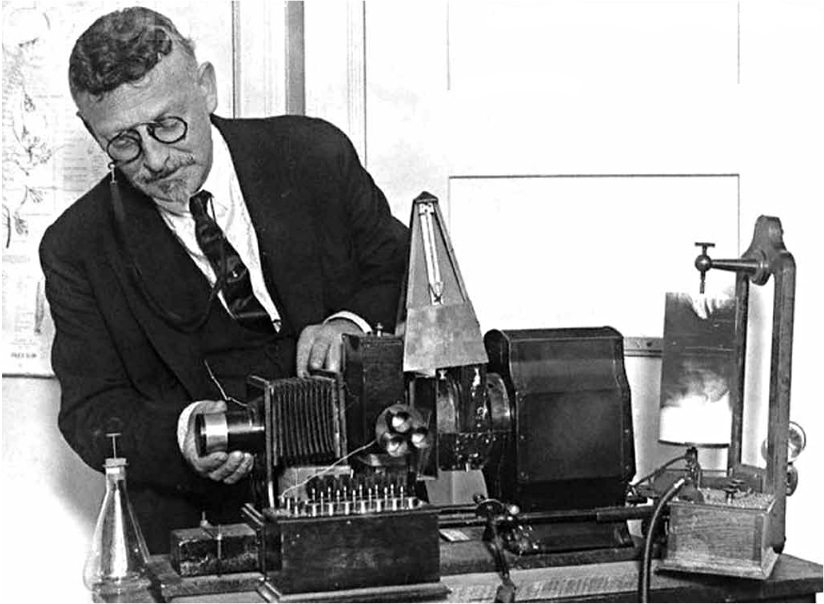 Abrams adjusting the machine (circa 1922)
Abrams adjusting the machine (circa 1922)
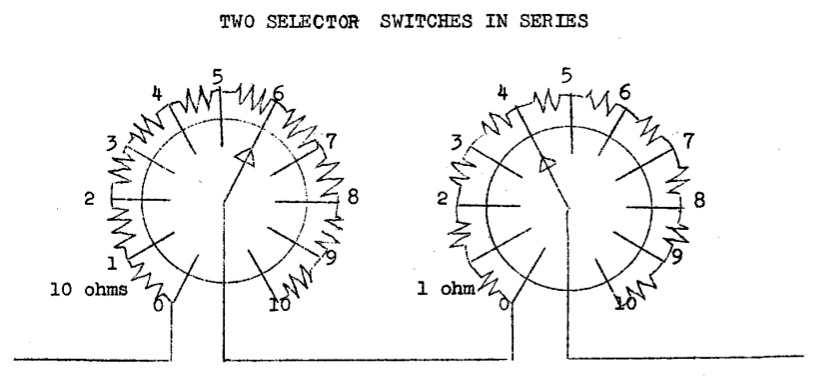
The use of rheostats for tuning, involved a problem of practical use. One could not be sure that a previous setting would be exactly duplicated in the future. Even with the aid of a pointer on the rheostat knob and a scale marked on the panel, there was always the possibility that the sliding arm on the rheostat would be set slightly higher or lower than before, when the operator wanted to duplicate a previous tuning. To eliminate this problem, the tuning mechanism was changed. Instead of rheostats, selector switches were adopted. Fixed resistances were connected between each adjacent pair of switch contacts, as shown in the diagram below. All resistances used between contacts of one rheostat were of the same resistance value, designated as ohms. In this way, use of the switch knob determined how many equal units of fixed resistance were placed in the circuit. For example, if the switch knob was turned to place the switch arm at position No. 5, then three of the fixed resistances were placed in the circuit. Similarly, if the switch knob was turned so as to place the switch arm at position No. 6, there would then be six units of fixed resistance included in the circuit. Usually the switches that were used gave a choice of 10 or 11 positions, numbered from zero to 9 or zero to 10. The resistances used had to be of the non-conductive type, and preferably of very close tolerance with respect to the resistance value.
Previously when rheostats were used, the rheostat dials were usually marked from zero to 100 in 1-unit or 2-unit steps. This range of 100 units could be duplicated by using two selector switches as shown in the diagram below — in place of a 100-ohm rheostat, the left-hand switch would have 19-ohm resistors between each adjacent pair of contact points, while the right-hand switch would have 1-ohm resistors between each pair of adjacent contact points. In this way, each resistance value from zero to 100, in steps of 1 ohm (the customary unit of electrical resistance measurement) could be included in the circuit by using the appropriate settings for the two switches. Correspondingly, two rheostats in series were replaced by four selector switches in series.
In an early period each resistance step was represented by a switch contact point mounted on a panel in the form of a screw having a large flat head. The heads were installed on the curve of an arc; the switch had a metal arm bent down at one end to make contact with the flat heads — the other end of the arm had a collar and set screw for attachment to the switch shaft or axle, which was rotated by a knob. Later this rather cumbersome arrangement was superseded by the use of rotary single-gang selector switches in which the arm and all contact points are contained inside the switch housing. From this housing protrude the contact connections and the shaft for changing the switch setting.
 Because of Dr. Abrams’ experience with tuning rates derived from the use of rheostats, he assumed that it was the quantity of resistance in the circuit which tuned the emanations coming from the human body, and from other organisms and types of matter. This assumption was accepted for many years by his followers and successors, but was later proven to be a fallacy. There was another factor in the use of the rheostat, which went unrecognized for many years. It will be discussed in a later installment, devoted to the theory of radionic tuning.
Because of Dr. Abrams’ experience with tuning rates derived from the use of rheostats, he assumed that it was the quantity of resistance in the circuit which tuned the emanations coming from the human body, and from other organisms and types of matter. This assumption was accepted for many years by his followers and successors, but was later proven to be a fallacy. There was another factor in the use of the rheostat, which went unrecognized for many years. It will be discussed in a later installment, devoted to the theory of radionic tuning.
MEASUREMENTS OF AMPLITUDE OR VOLUME
The inauguration of tunings for disease radiations as outlined previously in this series, was a major, even a revolutionary advance; but there was a further need — some means to determine the magnitude of each radiation detected. Before this was found, the operator could get some idea of the magnitude through variations in the apparent strength of the percussion reflex, but this was not at all specific and depended too much upon the interpretation of the operator.
It was then learned that once the tuning rate of an incoming radiation had been ascertained and placed on the instrument panel, another rheostat could be brought into use to find the relative strength of the radiation being detected. This auxiliary rheostat was used to extinguish the reaction — if the magnitude of the incoming radiation was small, a low setting of the rheostat would cause the reaction to disappear. If on the other hand the magnitude of the incoming radiation was large, then the rheostat would have to be advanced to a considerably higher setting, adding more resistance to the circuit, before the reflex action disappeared. Thus for the first time it became possible to measure disease radiation electronically!
MEASURING ORGANIC CONDITIONS
Later, when tunings were found for radiations from body organs, the measurement process was applied to the determination of extent of organ function, since the strength of radiation from an organ was found to be indicative of the condition of the organ and of its extent of function. Then the operator could determine which organs were functioning normally, which were below par in function (and just how much below par for each deficient organ) and which if any were functioning at an abnormally high rate (over-active).
For even more precise measurements of extent organ function, or of magnitude of disease radiation, two or more rheostats could be used in series, for example, a 100-ohm rheostat for gross measurements and a 1-ohm rheostat for fine measurements. The measuring rheostat or rheostats could be connected in series with the tuning rheostats, but had to be in a different position on the vertical (top to bottom) axis on the instrument panel from that occupied by the tuning rheostats. In other words, the measurement rheostats had to be placed either above or below the row of tuning rheostats — ordinarily they were placed below the rheostats used for tuning. If placed on the same horizontal row as the tuning controls, the rheostats intended for measurement purposes ceased to serve these purposes and instead became part of the tuning mechanism. It was possible also to use other than series connections between the tuning controls and the measurement controls, provided that the prerequisite of keeping the two types of controls on separate horizontal rows was observed.
When tuning rheostats were replaced with selector switches, some instrument makers continued to use rheostats for volume measurement purposes, while others replaced them with selector switches to which a series of fixed resistances were connected as with the tuning controls.
See Part II here.





Posted in Health, Other Topics, Science For The New Agewith comments disabled.